The new chair of a major review into medical training has pledged to bring the “dial up” system into the modern era. Professor Dame Jane Dacre has been appointed by NHS England and the Department of Health and Social Care to implement the Medical Education and Training Review, delivering change to UK’s creaking medical training […]
Author: tio
-
Vaccines Work. Here’s Why We Care About Your Unvaccinated Child.
While normal people don’t want any child to suffer or die because their parents were tricked by disinformation, the leaders of the anti-vaccine movement, who profit by lying about vaccines, don’t care at all.
The post Vaccines Work. Here’s Why We Care About Your Unvaccinated Child. first appeared on Science-Based Medicine.
-

Mourning on Schedule: How Grieving Became a ‘Mental Illness’
I wrote this poem five months after Ginny’s passing:
Waking Up
Every day
I wake up
And remember she’s not there
5 times a night
I wake up
And lose her yet again
Sometimes
In my dreams
She comes to me
It seems so real
And I rejoice
Until I wake up
And lose her yet again
Joy becomes pain
Yet I still want her to come
Even if it’s just a dream
She still loves me
Like she always has
Until I wake up
And remember.My wife, Ginny, died last April. Ten months ago.

I still cry almost every day. I often wish she were still here. I have dreams about her. I sometimes talk to her as if she can hear me. Things remind me of her, all the time, and when it gets to me, I cry again. It’s hard to get out of bed some mornings. I feel unmotivated, forgetful, and unable to think straight. I’m frequently tired but wake up multiple times a night and have trouble going back to sleep. I move and think much more slowly than normal for me.
I have sometimes wished I were dead. No plans to do anything, more the feeling that my life no longer seems worth living.
It would appear I have a “mental disorder.”
I meet the criteria for “Major Depressive Disorder”: depressed mood, sleep disturbance, loss of energy, cognitive impairment, and thoughts of death. Five of nine criteria for more than two weeks. I’m ill!
In another two months, unless things radically change, I will have a new mental disorder: “Prolonged Grief Disorder”! Here is the description: “A distinct mental disorder where the intensity and duration of grief symptoms are disabling and exceed social, cultural, or religious norms.”
According to the DSM, the “social, cultural or religious norm” for grieving in the USA is a year. Twelve months. Oh, only six months if you’re a child. I guess kids are supposed to “get over it” more quickly. Because they’re resilient, right?
Who decided that and how? We will find out a little later in this piece.
My Love Story
I grew up with a very hard-working, very emotionally distant mother, four brothers close in age, and a father who was away at work most of the time. I learned early on that love and affection were scarce commodities and that I’d better get used to fending for myself. I spent a lot of my early childhood alone, and pretended I liked it that way. But I was miserable and hated myself. I was incredibly shy and terrified of talking to a girl I liked, let alone asking her on a date!
Ginny and I met on our second day of college on a bike ride. It took me five more weeks to figure out she liked me and ask her out. She had to make it pretty obvious. I was pretty dumb about girls!
 Ginny changed all that. She loved me for who I was. She was my safe place, my true love, the person I could count on. We were together for 49 years. Married for 44. Raised three boys, went camping, backpacking, biking, played tennis, ping pong, card games, board games, watched movies together, laughed a lot, cried a lot, snuggled a lot, sometimes argued but always sorted it out by bedtime. We said we loved each other probably five times a day or more. When I needed love and support, I went to Ginny. She did the same with me.
Ginny changed all that. She loved me for who I was. She was my safe place, my true love, the person I could count on. We were together for 49 years. Married for 44. Raised three boys, went camping, backpacking, biking, played tennis, ping pong, card games, board games, watched movies together, laughed a lot, cried a lot, snuggled a lot, sometimes argued but always sorted it out by bedtime. We said we loved each other probably five times a day or more. When I needed love and support, I went to Ginny. She did the same with me.Ginny taught me to have fun. She taught me to love myself. She made it safe for me to love others fully. She was my life.
She died of cancer at age 66.
To say that I miss Ginny is the grossest of understatements. We used to talk all the time about being like her Auntie Til and Uncle Al — riding our bikes around into our 80s, seeing our grandkids have kids of their own, driving our RV around the country, visiting Canyonlands, Yellowstone and other parks around the country, and visiting our relatives on the East Coast (we lived in Olympia, WA). To lose her not only meant losing our companionship. It meant losing our vision of what our future would look like. It meant losing a huge part of my identity. It meant losing a big part of my purpose in being alive.
We never expected that Ginny would be the one to die first. We talked about it often. All the men in my family, both sides, died in their 60s or sooner of heart attacks, except my dad, who survived a heart attack at 40 and changed his lifestyle, and managed to make it to 85. But notwithstanding his amazing recovery story, we both figured I’d die first. On the other hand, the women in her family all lived into their 90s. There was no cancer on either side of the family. I was completely unprepared to still be here when she was gone. That was not how the story was supposed to go!
When Ginny died, I also lost my safe haven. I thought I had dealt with the attachment difficulties I noted above, but apparently, I had set them aside with the idea that I’d never have to deal with them, because I’d always have Ginny, and she’d always love me! When she died, a huge rush of these feelings unexpectedly came back on me with a vengeance. Now I was alone again, just like I was as a child. Fortunately, I’ve learned a lot of skills since then and have a pretty good network of genuine friends who have helped me move through this very painful time. And I was fortunate to find a very compassionate and competent grief counselor who has been seeing me for the better part of eight months now. But I am still alone much of the time, and it is very, very hard. I feel sad, angry, frightened, lonely, and sometimes wonder why I am still here and what it is I’m supposed to be doing. And I get tired. Existentially tired. Exhausted.
So does this make me “mentally ill?” Or am I just a person who misses someone they loved very much, and has to deal with the sadness of moving on alone? And how long am I permitted to take with that? When am I supposed to be “done” with grieving? How long is “too long”?

What is “Normal?”
So what is “normal grieving?” Let’s take a look at some social, cultural and religious norms for grieving around the world.
Here are some examples of what is considered normal grieving in different cultures:
- In Egypt, tearfully grieving after seven years would still be seen as healthy and normal.
- In traditional Vietnamese culture, mourning lasts two years, reflecting the deep respect for the deceased. During this time, family members may wear white or subdued clothing, avoid celebratory events, and offer daily prayers. A special ceremony is held after the two-year mark to signify the end of the mourning period.
- In Jewish tradition, shiva lasts seven days — an intensive mourning period where the community supports the bereaved. This transitions to shloshim (30 days) and eventually a year of saying Kaddish for close relatives. This graduated approach acknowledges that grief changes rather than simply ends.
- Chinese mourning traditions historically prescribed 100 days of intensive grief followed by a three-year mourning period for immediate family members.
- In Victorian England, widows were expected to observe strict mourning for two years, with specific clothing requirements that gradually relaxed as time passed.
- In Greek Orthodox tradition, a service is held on the first day after the funeral, the third day, the 9th day, the 40th day, every three months for the first year, and annually thereafter.
- Many Indigenous American tribes view grief as an ongoing relationship with the deceased rather than a process with a definitive endpoint.
- Similarly, in Mexican Day of the Dead celebrations, grief transforms into an annual reconnection with departed loved ones, suggesting that grief doesn’t end but evolves into meaningful connections that continue throughout life.
As we can see, expected grieving periods and rituals vary dramatically by cultural tradition. These expectations can vary from months to years to forever! So if you come from Egypt, does “Prolonged Grief Disorder” ensue at the one-year point? Or do you have to exceed seven years before you qualify?
How Long is “Too Long”?
Given this wide range of cultural practices and expectations, which is explicitly identified in the definition of Prolonged Grief Disorder above, how did they come up with the supposed norm of one year (and six months for those resilient little kids)? They held a “consensus conference.”
They couldn’t agree on the criteria, so they got together in a big committee, and then they reached a consensus. In other words, one year (and six months for children) is an agreement reached by a group of “mental health professionals” sharing their opinions and arguing about it until they agreed. Kind of like figuring out what movie we’re going to see or where we’re going to go for pizza tonight. Consensus. They might have voted on it.
I also have to wonder who the “stakeholders” were that were invited to the “consensus conference.” I’d bet my life savings there was no one there representing actual human beings who were going through this grieving process themselves.
So as far as I can make out, in two months, if things continue as they are, I will have a new “mental disorder,” because a bunch of psychiatrists got together at a conference in New York and decided, “OK, we’ve decided a year is long enough to grieve. A year? Everyone good with that? Any objections? OK, all in favor, say ‘Aye!’”
I shared this issue with my good friend Laurie, and she brought up an interesting question:
“If it’s a leap year, do you get an extra day?”
This question points out the utter absurdity of these “criteria.” Why would I suddenly stop missing Ginny or wishing she were here at the magical one-year mark? Why don’t people just get to be sad as long as they need to? And these poor kids! Their mom dies, or their dad or their sister, and they’re supposed to be substantially “over it” in six months?
Psychiatry’s explanation for this comes down to “being able to provide treatment” — in other words, to satisfy insurance companies that they ought to pay for services to help these people. From Miriam Solomon’s critique of “Prolonged Grief Disorder” being added to the DSM:
“… prolonged grief has symptoms (yearning for and preoccupation with the deceased) that are not shared by other disorders AND there is a new, targeted, grief therapy, developed by Katherine Shear (2005; 2014) that offers superior relief to those dealing specifically with prolonged grief.”
But why shouldn’t we just provide the necessary services, if desired, and bill the insurance company for an “adjustment disorder” or something more benign that doesn’t stigmatize the grieving process? Or better yet, change the whole approach so that a DSM code is not a requirement to receive “targeted grief therapy” or other forms of assistance?
Drs. Joanne Cacciatore and Allen Frances appear to agree with me:
“It would be preferable if US-based insurers did not predicate payment for supportive grief counselling on a medical code; this would be much more respectful of grievers. Many people, recognising that bereavement can be an intense exogenous stressor, want to leave grief, and grievers, safely out of the reach of well-meaning but intrusive doctors and treatments. Grief warrants strong social support and compassionate connection, not medicalisation.” [Emphasis added.]
The other thing to keep in mind is that most people are not offered Katherine Shear’s “new, focused grief therapy” once they are diagnosed. They are most commonly offered psychiatric drugs to “take the edge off” or “help them cope.” This, to me, adds insult to injury — not only are you telling me my feelings are abnormal and unacceptable, you’re telling me that there’s nothing I can do about them other than to take drugs to make me feel better. (Because that is the goal — to feel better! Not to find a new way to live your life, but to make those “bad feelings” go away. Talk about toxic positivity!) And we also know that such interventions often have unintended consequences that the grieving person has not been prepared for.
What is the US Cultural Norm?
The DSM is mainly used in the USA, so the assertion of one year as the “cultural norm” on which “Prolonged Grief Disorder” is based should be the US standard. But what do people in the USA regard as a normal course of grieving?
According to a recent Mad in America article, a study of grieving people stated that “Nearly every participant (98%) believed their response to loss was normal and understandable.”
I belong to several online support groups, including two Facebook groups for widows and widowers. There was a post recently on one of them about Prolonged Grief Disorder, entitled “Some people get stuck in grief — now scientists think they know why.” The reception from the grieving widows/widowers toward this posting was not very warm!
Some comments included:
- Almost 6 years since I lost my wife, so I guess I must have their disorder. I call it love…
- Grief has three stages…
1. The beginning.
2. The middle part.
3. The rest of your life.
Your person may be gone, but not the love. As long as you love your person, so long will you grieve. Period. Nothing strange, no disorder, just reality. - Prolonged grief happens when someone very close to you passes that you interacted with on a daily or routine basis. That’s why… deep love means deep grief.
- Grief has no expiration date. I’ve never thought “I can’t wait until I no longer grieve for my son or my parents.” I grieve because I love them and I’ll forever miss them being present in my life.
- Grief is the price of love.
- Grief is not a disorder. It’s not getting stuck in grief, we carry grief with us. It becomes part of our lives. We learn to live with it and it’s different for everyone.
- I wonder if any of the scientists doing this research have ever experienced grief! Based on my own grief and all of these comments, seems we all feel like our grief is “normal.”
These commenters were mostly in the United States. This is what our cultural and social norms really are, at least among people who are actually grieving! Not a few weeks, not a few months, not a year — grieving takes however long it takes for that person, and for some, it is a lifetime. It’s not something you get over or move past, like losing that car you really loved or having to move to a new house. A part of you is gone, and you have to learn to create a new life for yourself that includes the fact that they are no longer there. As a wise young man recently said to me, “If your arm were amputated, other people could hand you things. But they can’t give you back your arm.” The grieving person cannot “return to normal.” A part of them is missing that can’t be replaced.
While the Facebook groups of people who are actually experiencing grieving seem to show a complete willingness to accept that grieving is an ongoing process that may take years or never be “done,” the general population in the USA has increasingly been inundated with the message from the mental health system that grieving is a “mental health issue” (hence not something they are qualified to deal with), and that people really should “recover” from grief in a “reasonable” timeframe. Additionally, as there is no formal grieving process generally recognized in the USA, there is a lot of uncertainty as to what IS normal. This often leads to discomfort discussing the subject, and it’s a very human tendency to avoid uncomfortable discussions, because they are, well, uncomfortable! This unfortunately dovetails all too well with recent efforts to market the concept of “Prolonged Grief Disorder” and is making it harder for folks to have simple and honest discussions about what grieving is really like, especially when the grieving person continues to struggle months or even years into the process.
In the next section, we’re going to take a look at how to challenge some of these assumptions and to become more in tune with what is actually helpful to a person who has experienced a major loss in their life.
Grief Education
We all should do our best to provide what love and support we can to a grieving person, knowing that however much we give, it won’t be enough to make it all better. But this support is very much needed and will still be appreciated.
Here are some things we can do that might really help:
- Listen, ask questions, and connect with them. You can’t fix it, but you don’t need to and shouldn’t try. Efforts to “help them feel better” generally come off as invalidation or “toxic positivity” (the need for them to be “positive” in order to make you feel better). Instead, let them tell you how the experience has been for them, and acknowledge them for having the courage to share their feelings with you.
- Expect a wide range of emotions. We all expect sadness, but some unexpected emotions are anger (at their partner for leaving, at themselves, at the world, at God), relief (usually if someone was suffering, but sometimes because of a conflicted relationship), guilt (especially for being angry and/or feeling relieved!), or confusion (Why did this happen? Did I cause it? Could I have prevented it? Did I deserve it?). Really, any human emotion can come up, and all are OK for a person to experience.
It is also very common for mourners to think about dying as a way to escape the pain or to rejoin their loved one in the afterlife. This is normal and not a cause for alarm! Make it safe for them to tell you about what they are experiencing, and do your best to let them know how totally understandable their feelings are. - In almost every case of serious grieving I’ve seen, including my own, an interesting phenomenon occurs. At first, everyone wants to offer their help: “What can I do?” “Call me any time!” “You know I’m there for you!” But as time goes along, the mourner’s support network gradually shrinks. Not because people don’t care, but because people’s lives get in the way, and compassion fatigue takes over, and sometimes it’s just hard to keep hearing that this person you care about continues to suffer and what you have done doesn’t seem to be enough. There is a tendency to stop checking in, to drift away assuming or hoping things are “better,” or to move again into toxic positivity, because it would feel so much better if the person you care about would just be happy again! And this often happens just as the hard reality of the permanency of this loss is beginning to truly sink in. Don’t drift away after six months — they may need more support now than they did immediately afterwards! Take some extra time to check in with them now that the initial outpouring of support has passed.
- As time has gone along, I have sometimes gotten subtle spoken and unspoken messages from some people that this topic is making them uncomfortable and that I need to “be more positive” or “give my pain to God” or “find a way to be happy.” This has led me to be more cautious about sharing what’s going on, as I am beginning to have the expectation that my actual answer to “How are you doing today” is not going to be welcome! So the grieving person, when asked, might say, “I’m doing OK” or “I’m fine,” even if they are struggling mightily, because our culture seems to be telling us that it’s time to be done or at least handle this stuff by yourself now — people are getting tired of it! Don’t accept this kind of answer at face value. If someone says, “I’m doing OK,” please invite them to expand on that. “What’s OK looking like for you right now?” or “I can imagine things are still rough for you sometimes. I’m here to listen if you want to share.” Make it easy for the person to hear that you are OK with them continuing to feel sad or angry or whatever is going on, and that you don’t expect them to be OK!
- Be affectionate, to the degree that the person is comfortable with it. One question often raised on the Facebook support groups is, “Where do you go to get a hug?” If the person was in a very affectionate relationship (as I was), this lack of contact can be very painful, and a well-timed hug or a holding of hands or a firm shoulder grab can show solidarity in a way no words can convey. Of course, some people are uncomfortable with affection from other people for various reasons, and that has to be respected, but for many, the more hugs, the better!
- This is a time when new spiritual realities may awaken in a person. I have had several lucid dreams (where I know that I am dreaming but don’t awaken) where Ginny has come to visit me. Before this, I experienced lucid dreaming once every five to ten years or so. After her death, I experienced lucid dreaming with Ginny five to six times in a few months! In one such dream, I asked her what it was like. She said it was really nice, they had groups and classes and everyone ate meals together, but the best part was that everyone seemed to get along, no one was ever upset with each other.
I truly believe it was her visiting me from whatever afterlife she was experiencing. This has dramatically altered my view of what we are as spiritual entities.
Some might say I’m psychotic for believing this. But it’s common for people to have visitations in one form or another. And it’s very common for people who have lost someone important to need spiritual guidance to make sense of the situation. Don’t be afraid to get into this area of discussion with them, and don’t be surprised if they put forward some new beliefs or difficult questions that they may not have concerned themselves with before. It can be challenging to incorporate the implications of this kind of loss into our spiritual worldview. - And for God’s sake, don’t diagnose them or tell them “you should get some help!” By no means should you expect them to be “done grieving” at a year, or at any given time. Their loss will be with them for the rest of their lives, and there is nothing “mentally ill” about it. It’s certainly OK and sometimes very helpful to get some more formal support, such as a support group or a grief counselor, but everyone is different, and let’s be honest, not all counselors are equipped to really provide the kind of support I’m describing here. So don’t prescribe solutions — ask them what they think will be helpful, and listen carefully to the answers!
Bottom line: it is not reasonable or rational to expect a grieving person to “return to normal.” Normal is no longer possible. The best we can do is to start to develop a new “normal” that includes the painful knowledge that the person we loved so much is no longer going to be present in the same way.
Remember also that grief occurs for many, many reasons besides the death of a life partner. Any time someone appears to be in distress, don’t be afraid to ask and find out what is going on, and keep in mind that grief and loss are often at the bottom of many “mental disorder” manifestations. It’s a big part of what makes us human.
I wrote this poem nine months after Ginny’s death. I think it communicates how regardless of the support one might receive from friends and community, the personal experience of loss remains excruciatingly painful.
Leftovers
You get to have the stuff
Nobody else wants
The bones, the gristle
The skin, the fatNo one wants the chicken’s neck
Or the cow’s hoof
Or the ox’s tail
(maybe in some soup)You can have what no one has a use for
Your life is leftovers
Just enough to live on
Enough to keep you alive
Though why, no one can saySo you wait for crumbs of love to
Fall from the table
Gobble them up hungrily,
Knowing it’s all you getYou used to have big
Sumptuous meals
All the love you can eat
The good stuff every dayBut one day
Somehow
It was taken away from youNow you are supposed to be happy
With the leftoversI’m hungry!!!
****
Editor’s note: first published on Mad in America March 12th 2026
Mad in the UK hosts blogs by a diverse group of writers. The opinions expressed are the writers’ own.
The post Mourning on Schedule: How Grieving Became a ‘Mental Illness’ appeared first on Mad in the UK.
-
Oscar Winner ‘One Battle After Another’ Sees Piracy Surge, While ‘Sinners’ Stays Flat
In 2007, The Pirate Bay supported “OscarTorrents,” which aimed to be a pirates’ counterweight to Hollywood’s annual awards show.
At the time, mass movie piracy was still a fringe activity, with no instant streaming options available. Nonetheless, more than 100,000 ‘pirates’ voted for their own movie favorites.
While the OscarTorrents project was a clear display of defiance, the outcome of the voting was rather mainstream. The Departed was crowned ‘Best Picture’ in the official Oscars ceremony, as well as in the pirate equivalent, and many of the other winners were also identical.
2026 Oscars
Fast forward nearly two decades, and the annual awards ceremony continues to make an impact. Typically, the winner of the Oscar for ‘best picture’ will see a boost in downloads on torrent sites and elsewhere.
Based on a sample of torrent activity tracked by IKnow, we can report that pirated downloads of “One Battle After Another” tripled the day after the awards ceremony compared to the week before. The chart below shows the daily estimated downloads for five of the Oscar nominees, with the winner clearly standing out.
Piracy Impact: 2026 Oscar Season 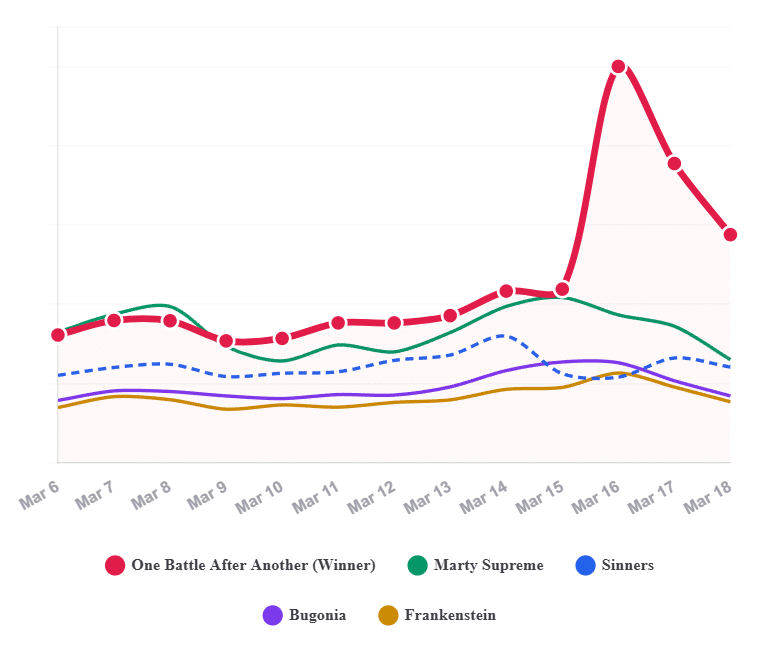
This Oscar winner’s surge doesn’t come as a surprise, as we have seen this play out before. While there is always a boost for the best picture winner, relatively speaking, this is typically greater for lesser-known films.
The 300% increase for “One Battle After Another” is larger than that of “Oppenheimer” in 2024 but less pronounced than the quadrupling of last year’s winner, “Anora”.
No Piracy Boost for Sinners
What’s more surprising in this year’s data is the absence of an Oscar boost for Sinners, which was one of this year’s favorites with a record number of sixteen nominations. The film won four Oscars last weekend, but this didn’t trigger any new activity on pirate sites.
Sinners already saw its downloads on pirate sites triple in January after the nominations were announced. The nominations surge in January appears to have already satisfied pirates’ demand.
In the piracy data sample, we also see the lack of an Oscar effect for “Marty Supreme,” which did not see any increase in interest either. That is less surprising, of course, because the film failed to win any Oscars despite receiving nine nominations.
That said, it is not only the best picture winner who enjoys a boost in pirate downloads. While less visible in the chart above, “Frankenstein” and “Bugonia” also saw temporary download spikes of close to 50%, which can be attributed to the Oscar night spotlight for these titles.
Legal Demand Rises Too
The piracy boosts observed here are typically the result of an overall increase in demand. Legal streaming platforms tell a similar story, although not the same. Streaming search engine JustWatch informs us that, with a 231% increase, “One Battle After Another” was also the big winner in terms of legal demand.
Interestingly, Sinners did get a boost in interest on legitimate streaming platforms. JustWatch reports that Sinners saw an increase of 136% following the Academy Awards. JustWatch’s data is based on activity from U.S. users but, even when looking at U.S. traffic alone, a similar piracy effect could not be observed on our end.
Legal Streaming Impact: 2026 Oscar Season 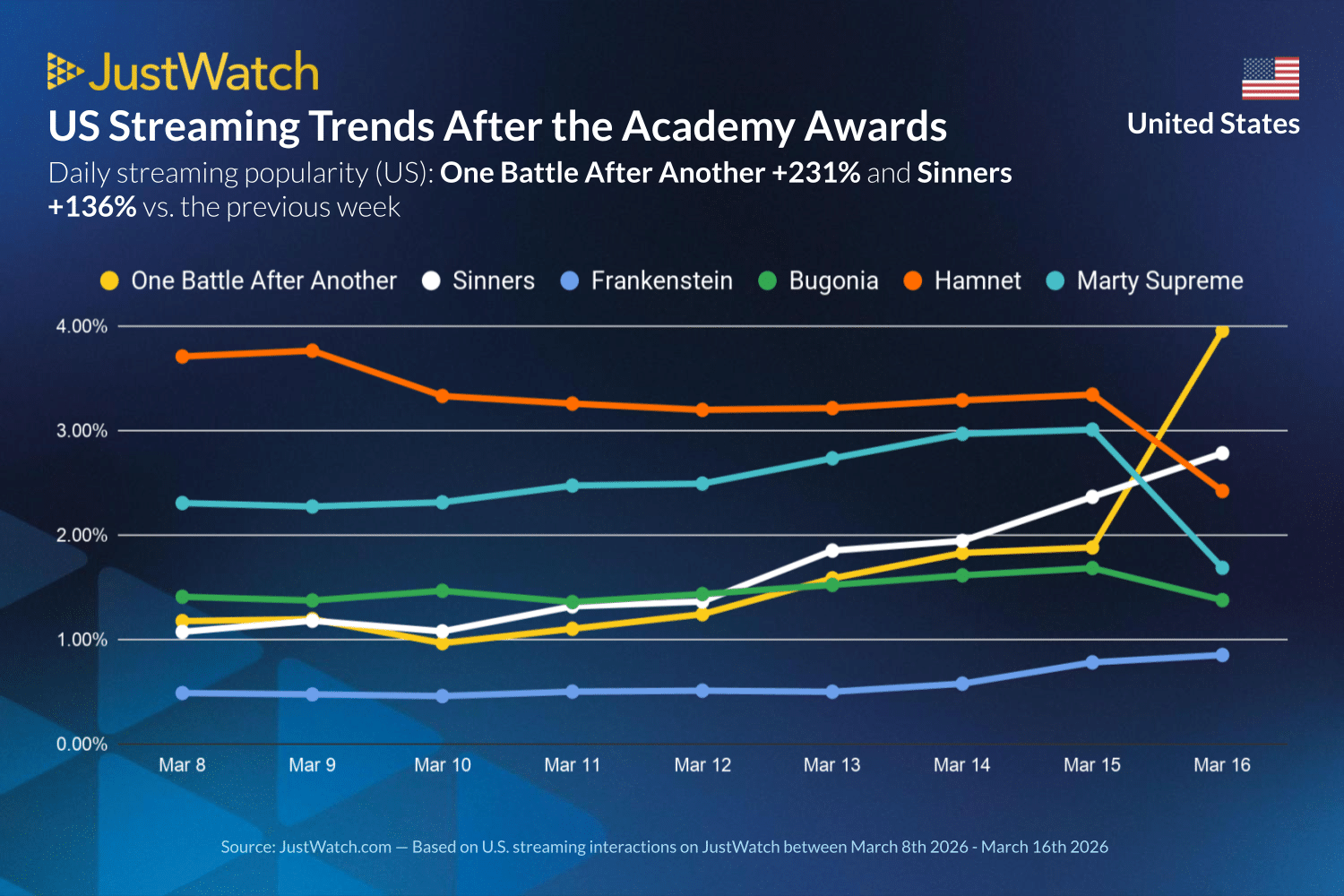
The graph above shows that legal demand for Marty Supreme through streaming platforms clearly dropped. That’s also different from our findings, as demand on pirate sites remained stable.
As with all trends today, these media-triggered spikes in demand don’t tend to last very long. After the initial boost on Monday, the piracy interest for most titles immediately started to level off. That said, with an Oscar for best picture in the bag, the status of “One Battle After Another” will remain permanently elevated.
—
Note: The data used in this article comes from Iknow, which tracks torrent downloads through DHT and PEX. While it may not be able to track all downloads, it’s a substantial sample. This sample only looks at torrent downloads. Views on streaming platforms, direct downloads, and other piracy sources can’t be measured directly. That said, we assume that the trend will be similar there.
From: TF, for the latest news on copyright battles, piracy and more.
-
Feds Disrupt IoT Botnets Behind Huge DDoS Attacks
The U.S. Justice Department joined authorities in Canada and Germany in dismantling the online infrastructure behind four highly disruptive botnets that compromised more than three million Internet of Things (IoT) devices, such as routers and web cameras. The feds say the four botnets — named Aisuru, Kimwolf, JackSkid and Mossad — are responsible for a series of recent record-smashing distributed denial-of-service (DDoS) attacks capable of knocking nearly any target offline.
Image: Shutterstock, @Elzicon.
The Justice Department said the Department of Defense Office of Inspector General’s (DoDIG) Defense Criminal Investigative Service (DCIS) executed seizure warrants targeting multiple U.S.-registered domains, virtual servers, and other infrastructure involved in DDoS attacks against Internet addresses owned by the DoD.
The government alleges the unnamed people in control of the four botnets used their crime machines to launch hundreds of thousands of DDoS attacks, often demanding extortion payments from victims. Some victims reported tens of thousands of dollars in losses and remediation expenses.
The oldest of the botnets — Aisuru — issued more than 200,000 attacks commands, while JackSkid hurled at least 90,000 attacks. Kimwolf issued more than 25,000 attack commands, the government said, while Mossad was blamed for roughy 1,000 digital sieges.
The DOJ said the law enforcement action was designed to prevent further infection to victim devices and to limit or eliminate the ability of the botnets to launch future attacks. The case is being investigated by the DCIS with help from the FBI’s field office in Anchorage, Alaska, and the DOJ’s statement credits nearly two dozen technology companies with assisting in the operation.
“By working closely with DCIS and our international law enforcement partners, we collectively identified and disrupted criminal infrastructure used to carry out large-scale DDoS attacks,” said Special Agent in Charge Rebecca Day of the FBI Anchorage Field Office.
Aisuru emerged in late 2024, and by mid-2025 it was launching record-breaking DDoS attacks as it rapidly infected new IoT devices. In October 2025, Aisuru was used to seed Kimwolf, an Aisuru variant which introduced a novel spreading mechanism that allowed the botnet to infect devices hidden behind the protection of the user’s internal network.
On January 2, 2026, the security firm Synthient publicly disclosed the vulnerability Kimwolf was using to propagate so quickly. That disclosure helped curtail Kimwolf’s spread somewhat, but since then several other IoT botnets have emerged that effectively copy Kimwolf’s spreading methods while competing for the same pool of vulnerable devices. According to the DOJ, the JackSkid botnet also sought out systems on internal networks just like Kimwolf.
The DOJ said its disruption of the four botnets coincided with “law enforcement actions” conducted in Canada and Germany targeting individuals who allegedly operated those botnets, although no further details were available on the suspected operators.
In late February, KrebsOnSecurity identified a 22-year-old Canadian man as a core operator of the Kimwolf botnet. Multiple sources familiar with the investigation told KrebsOnSecurity the other prime suspect is a 15-year-old living in Germany.
-
Phantom Contracts and Kickbacks: Poland’s Judicial Corruption Scandal Widens
Polish authorities on Thursday detained five court officials in a widening investigation into a multimillion-dollar embezzlement scheme at the Kraków Court of Appeal, marking a new chapter in one of the largest judicial corruption scandals in the country’s history.
The arrests signal that the sprawling graft network, which has already led to dozens of indictments, continues to be an active target for law enforcement.
According to Poland’s Central Anti-Corruption Bureau (CBA), the latest suspects include a deputy director, the head of the court’s IT department, a chief procurement specialist, an acting deputy chief accountant, and an IT specialist. Prosecutors accuse them of operating as an organized criminal group within the judicial system.
The investigation centers on allegations of bribery, fraud, and money laundering used to siphon off public funds. The total losses linked to the broader Kraków court scandal are estimated at nearly 35 million zloty, or about $9 million.
According to the anti-corruption bureau, the fraud relied on a network of fictitious consulting and IT contracts. Companies bound to court insiders by family, social, and financial ties were awarded regular contracts to produce analyses, studies, and IT services that were never actually performed.
To create the illusion of legitimate services and establish a paper trail, the supposed tasks were allegedly reassigned to existing court employees. Once the state paid the outside contractors, portions of the funds were secretly funneled back to court officials as illegal kickbacks.
Thursday’s detentions are not an isolated crackdown. The CBA noted that this specific investigative strand has already yielded a steady drumbeat of arrests in December, February, and March.
The enforcement actions run parallel to a massive, ongoing legal reckoning. In April 2025, a landmark trial opened in the city of Rzeszów involving 43 defendants. Prosecutors in that case outlined a vast criminal organization, allegedly led by the court’s former director, that embezzled state funds through bogus contracts and shell companies between 2001 and 2016.
In total, 57 people were initially indicted across several related dockets. The latest wave of arrests underscores that the scandal involves a deeply entrenched, multi-layered network rather than a single, contained conspiracy.
-
Profiting From Atrocities: The Russian Civilians Running a Lucrative Market for War Snuff
Russian Telegram channels dedicated to broadcasting graphic war footage from Ukraine—including apparent executions and the mutilation of corpses—have morphed into a highly profitable online industry operated in part by civilians and teenagers, according to a new investigation.
The independent Russian news outlet IStories analyzed more than 50 channels focused on war snuff. The investigation revealed that administrators draw tens of thousands of followers, monetizing extreme battlefield violence through advertising, cross-promotion, direct donations, and paid access to uncensored material.
Rather than frontline soldiers sharing the realities of combat, the networks are predominantly managed by opportunists hundreds of miles away from the trenches, turning atrocities into a lucrative digital enterprise.
The Factory Worker’s Side Hustle
One prominent example highlighted by the investigation was “Video *** 18+,” a Telegram channel that amassed nearly 40,000 subscribers.
IStories identified the channel’s founder as Vladimir Grebennikov, a 36-year-old refractory worker at an aluminum plant in Volgograd. Based on the channel’s posting volume, audience reach, and current market rates, the outlet estimated the operation could generate roughly 200,000 rubles a month in advertising revenue—a significant income in provincial Russia.
By early 2026, Grebennikov had reportedly sold the channel, citing burnout from managing the relentless stream of gore.
A Teenage Enterprise
Grebennikov’s operation, however, was far from isolated. The investigation exposed a disturbing demographic trend among the administrators: a significant number of them are minors.
One major snuff channel, boasting nearly 110,000 subscribers, explicitly listed teenagers as its advertising contacts. IStories identified Denis Bogolyubov, now 19, who was handling ad sales for the channel in 2023 when he was just 16. Another teenager, Artem Prigodin from the Arkhangelsk region, was also linked to selling ads for graphic “18+” channels while still underage.
Elsewhere, the outlet identified 18-year-old Artem Filippov from Kaluga as the founder of a separate graphic channel, which he appears to have launched when he was about 15.
Investigators located at least four other administrators who are currently no older than 15. One of them, a 14-year-old schoolboy from Abakan, heavily utilized Russian military imagery on his accounts and had reportedly applied to join Yunarmiya, the Kremlin-backed patriotic youth movement.
Crowdfunding Atrocities
The monetization tactics extend beyond traditional advertising. The investigation found that some channels openly solicit funds from their audiences to pay for exclusive violent content.
In one chilling instance, an administrator sought donations to purchase footage showing a wounded Ukrainian soldier being executed. The administrator later publicly thanked a subscriber for financially supporting the Russian fighter who provided the video.
While these channels exist primarily to traffic in gore and generate profit, human rights advocates and international investigators note they are inadvertently serving a second purpose: the vast trove of graphic material they circulate may ultimately serve as critical documentary evidence in future war crimes prosecutions.
-
This New Wave of Anti-Trans Legislation Threatens Us All
I was born and raised in Kansas. This is not something that I bring up often, because it’s a bit of a bummer. When I do tell people this, it usually elicits a reaction along the lines of “oh, I’m sorry”; a blank stare in disbelief that people do, in fact, live in Kansas; or a story about how they have some random second cousin that moved there and that, no, they are not planning to go visit.

-
They Didn’t Want to Have C-Sections. A Judge Would Decide How They Gave Birth.
On the afternoon of Sept. 9, 2024, Cherise Doyley was in her 12th hour of contractions at the University of Florida Health hospital in downtown Jacksonville when a nurse came in with a bedsheet and told her to cover up. A supervisor brought a tablet to Doyley’s bedside. Gathered on the screen in a video conference were a judge in a black robe and several lawyers, doctors and hospital staff.
“It’s a real judge in there?” Doyley asked the nurse at the beginning of what would be a three-hour hearing. “Now this is the craziest thing I’ve ever seen.”
Doyley hadn’t asked for the hearing. The hospital had sought it. Doyley had mere minutes to prepare. She had no lawyer and no advocate — no one to explain to her what exactly was going on.
Judge Michael Kalil informed her that the state had filed an emergency petition at the hospital’s behest — not out of concern for Doyley, per se, but in the interest of her unborn child. He described the circumstances as “extraordinary.”
The hospital and state attorney’s office wanted to force Doyley to undergo a cesarean section. Doyley, a professional birthing doula, didn’t want that and had been firm about it. She’d had three prior C-sections, one that resulted in a hemorrhage, and hoped to avoid another serious complication and lengthy recovery. She was aware that doctors were concerned about the risk of uterine rupture, a potentially deadly complication for her and her baby. She would say during the hearing that she understood the risk to be less than 2% and didn’t want to agree to a C-section unless there was an emergency.
But the choice would not be hers. The judge would decide how she would give birth.
Mentally competent patients typically have the right to choose their medical care — or refuse it. But there is one notable exception: pregnant patients. That inconsistency is particularly striking in Florida, a state that has pushed to expand medical freedom for those who wish to avoid vaccines or fluoridated water, while constricting the rights of people in various stages of pregnancy.
“There aren’t any other instances where you would invade the body of one person in order to save the life of another,” said Lois Shepherd, a bioethics expert at the University of Virginia School of Law.
In Florida and many other states, court-ordered medical procedures are just one of the ways pregnant patients’ rights are restricted. The effort to chip away at those rights is rooted in the concept of fetal personhood — that a fetus has equal and, in some cases, more rights than the woman sustaining it.
The hospital and state attorney’s office wanted to force Doyley to undergo a cesarean section.
The link between fetal personhood and court-ordered C-sections dates back to the 1980s, when courts started ruling that hospitals can override patients’ decisions in favor of the health of unborn children.
In the years since, proponents of fetal personhood began to push for even broader legal protections. In 1986, Minnesota was the first state to recognize fetuses as victims in homicide cases. Some states have imprisoned pregnant women for exposing their fetuses to drugs. Nearly 30 states have passed laws that allow hospitals to invalidate pregnant patients’ advance directives, which outline the kinds of life-sustaining treatment a person wants after a catastrophic illness or accident. At least one, Alabama, extended the concept of personhood all the way to the earliest stages of fertilization and conception by giving frozen embryos the same legal status as children, though the Legislature later said the law couldn’t be enforced.
And the fetal personhood movement has accelerated in the past several years, supercharged by the U.S. Supreme Court decision to reverse the abortion rights that had been protected by Roe v. Wade.
Florida has long been at the forefront of fetal personhood policies. The state was one of the first in the country to prosecute a woman for “delivering” drugs to her fetus during pregnancy in 1989, although the Florida Supreme Court later overturned her conviction. And after advocates twice failed to get a fetal personhood amendment on the state ballot, the Legislature is now considering a bill that would enshrine the concept in state law by giving embryos and fetuses the same legal status as people in wrongful death suits.
For women in labor, the potential impact of the bill is clear: Experts anticipate their medical needs could be further diminished in favor of their fetuses’.
Several legal experts told ProPublica they are alarmed by Doyley’s case and the legislation’s potential to allow for more court interventions during childbirth. Lawyers who represent women in fetal personhood cases already have identified a higher number of forced C-sections in Florida than other states.
The state attorney’s office for the 4th Judicial Circuit declined to comment on Doyley’s case, saying a response would violate her medical privacy. But in an email, a spokesperson noted why, in general, the office would intervene: “The courts have held that the State has a compelling interest in the preservation of the life of an unborn child and the protection of innocent third parties who may be harmed by the parental refusal to allow or consent to life-saving medical treatment.”
C-sections account for nearly a third of all deliveries in the United States. They can be necessary when babies are in breech position, the wrong orientation for birth, as well as in cases of maternal or fetal emergency. But in other cases, such as slow laboring or prior C-sections, the need for the surgery is less clear.
Surveys have found that more than 10% of women feel pressured into C-sections and other procedures by doctors worried about injuries to the baby. Patients generally don’t challenge doctors who say they’re necessary, and it is uncommon for someone to hold out and for a hospital to turn to the courts.
Florida has long been at the forefront of fetal personhood policies.
It is so rare, in fact, that advocates for the rights of pregnant women were shocked to discover that the same thing that happened to Doyley had happened to another Florida woman just a year and a half earlier.
The similarities in their cases were striking. Both women had had three prior C-sections. They had questioned the need for their previous surgeries and arrived prepared to fight for vaginal births. And both women were Black.
They had argued that compelling them to have C-sections violated their rights to make medical decisions. Hospital staff said the women’s medical decisions threatened the health of their fetuses. It would be up to the courts to decide which one mattered more.
Asked to consider the constitutionality of court-ordered C-sections, the U.S. Supreme Court declined in 1994, leaving a patchwork of decisions that vary by state.
In the early 1980s, a hospital in Georgia won a court order to force a woman with a dangerous pregnancy complication to have a C-section. Then, in 1987, a judge in Washington, D.C., approved a request to perform surgery on a pregnant woman dying from cancer without her consent. Later, a higher court reversed that ruling and held that hospitals should not override medical decisions. An Illinois appellate court in 1993 refused to order a woman to undergo a C-section.
Not long after, a patient named Laura Pemberton, who did not want a C-section, left a hospital in Tallahassee, Florida, against medical advice. A local judge sent law enforcement to her house to bring her back. Once she returned to the hospital, the judge ordered her to have a C-section, which doctors carried out. She later sued in federal court and lost. The 1999 decision by a federal district judge found that the state had a right to override her wishes.
“Whatever the scope of Ms. Pemberton’s personal Constitutional rights in this situation, they clearly did not outweigh the interests of the State of Florida in preserving the life of the unborn child,” the decision said. The decision marked a legal turning point in prioritizing fetal rights over the religious freedom and bodily autonomy of the mother.
In 2009, Samantha Burton arrived at the same hospital after going into premature labor at 25 weeks, in her second trimester of pregnancy. Doctors told her she needed to remain on bed rest, but she wanted to leave and go home to her children. The hospital got a court order for her to remain in the hospital and undergo any treatment doctors deemed necessary to save the fetus. She had an emergency C-section, and the baby was stillborn.
She appealed the ruling granting the emergency order, and a Florida appeals court ruled in her favor. It said the Circuit Court judge should have required the hospital to prove the baby was viable before imposing unwanted treatment, but the court stopped short of saying it was unacceptable to override the medical decisions of pregnant women in all situations.
Pregnancy is the only condition where Florida courts have ruled that a patient can be forced to undergo unwanted treatment. Even a state prisoner on a hunger strike has more rights to make medical decisions.
Those rulings give the state vast control over pregnant women.
“All of it essentially is about the state’s ability to decide that a fetus, at any point during a pregnancy, is more important than the person who’s pregnant,” said Rutgers University law professor Kimberly Mutcherson.
In March 2023, more than a year before Doyley’s court-ordered C-section, Brianna Bennett arrived in labor at Tallahassee Memorial Hospital — the same hospital where the women in the 1999 and 2009 lawsuits had given birth.
Those rulings give the state vast control over pregnant women.
Over the preceding years, Bennett had come to question the medical reasoning behind her three prior C-sections. Each recovery had been harder than the last, leaving her so incapacitated after the third that for two weeks she couldn’t even go to the bathroom without help.
By Bennett’s fourth pregnancy, her mother’s hip problems had gotten so bad that she needed a wheelchair and required some help from Bennett to function. When she went into labor, Bennett did not think she could care for all her family members while in recovery from abdominal surgery, so she insisted on trying for a vaginal birth.
Tallahassee Memorial Hospital had specialists on staff and a neonatal intensive care unit equipped to serve critically ill babies. Bennett believed it offered the kind of support she needed to be able to follow her birth plan. The hospital has handled a lot of high-risk pregnancies.
As Bennett’s labor stretched past 24 hours, a doctor confronted her about agreeing to a C-section, Bennett said. She continued to refuse, so the hospital reached out to the state attorney. In an email, Jack Campbell, state attorney for the 2nd Judicial Circuit, responded that the court needed to act quickly.
“I plan to file an emergency motion with the Court to allow TMH to take whatever steps medically necessary to protect the life of the child and mother,” he wrote.
During the hearing, 15 to 20 people squeezed into Bennett’s hospital room. As would later happen with Doyley, she found herself in front of a tablet with a judge on the screen.
Bennett said she found it offensive that so many people were concerned about the method of her delivery without taking into consideration how difficult it would be to take care of both herself and her baby while recovering from a C-section. “Are any of you gonna help me bathe or shower? Are you gonna help change my pad? Are you gonna help lift the baby out of the bed and put me in the bed because I can’t lift my legs? Is anyone going to help me?”
Campbell told ProPublica that he felt the hearing was necessary to save two lives, Bennett’s and her baby’s. “I’m real comfortable with what we did here,” Campbell said. “I hate the fact that she’s upset about it.”
A spokesperson for Tallahassee Memorial Hospital declined to comment on Bennett’s case, even though she signed a waiver allowing the hospital to do so. “We will not be able to discuss specific patients or cases,” the spokesperson wrote in an email. The hospital did not respond to questions about its history of seeking court intervention in multiple women’s medical decisions while giving birth.
Bennett said she tried to remain calm, but inside she was panicking. During the hearing, her baby’s heart rate spiked. The judge ordered her to have a C-section, and doctors wheeled her into surgery. The operation lasted 2½ hours and the surgical team had to cut around existing scar tissue and avoid her bladder. Her incision looked like an upside-down T and required a wound vacuum, a portable machine that helps incisions close more quickly.
She said a doctor who visited her room during recovery told her she should never get pregnant again, according to a civil rights complaint filed with federal regulators.The complaint is still under investigation, but lawyers for Bennett said they haven’t heard from investigators in more than a year. The U.S. Department of Health and Human Services did not comment on the complaint.
Bennett said she tried to remain calm, but inside she was panicking.
“I cried every single day,” Bennett said. “I felt like I was supposed to be happy. I’m supposed to be thankful that I have a new life and that the Lord has blessed me to see this new baby. And I’m not even happy.”
A year and a half later in Jacksonville, Doyley faced a situation eerily similar to Bennett’s.
She noted as her hearing began that she was the only Black person on the screen. About a dozen faces, most of them white, had gathered to challenge her medical decisions. She said it made her feel as if her race had something to do with the fact that she was thrust into the intrusive hearing.
“I have 20 white people against me, and because I am informed and I am making an informed decision, they are trying to take my rights away from me by force,” Doyley told the people on the screen, requesting a Black nurse or doctor.
“I don’t find that race really has much to do with this, ma’am,” the judge responded.
Dr. Erin Burnett said during the hearing that she did not think Doyley could successfully give birth vaginally because she had a history of stalled labors. A long labor after prior C-sections could increase the risk of uterine rupture, which could kill Doyley and the child, she said.
She said the baby’s heart rate showed some signs of distress and told Doyley it would be better to have a C-section before it became an emergency. If the baby’s heart stopped or if she lost oxygen during delivery, the baby could suffer a brain injury or death.
Dr. John Davis, the chair of the obstetrics and gynecology department, testified that the hospital had been recognized for its low C-section rate and did not perform unnecessary surgeries. Doyley’s condition required intervention, he said.
Burnett and Davis did not respond to requests for comment and the hospital declined ProPublica’s requests to interview them and others involved in Doyley’s care. Doyley signed a waiver allowing the hospital to discuss her case with ProPublica, but a spokesperson for University of Florida Health in Jacksonville would not comment, citing patient privacy. Nor did the hospital respond to questions about Doyley’s claim that race played a role in the decision to involve the court.
The research on the risks of uterine rupture after prior C-sections is unclear. Studies have found that 0.15% to 2.3% of these labors resulted in a rupture, depending on a number of factors such as body mass, a history of successful vaginal births and whether the labor was spontaneous or had to be induced.
Doyley, who felt comfortable with her odds and wanted to continue laboring, argued during the hearing that C-sections carry their own dangers — including a risk of death.
“A lot of that comes from medical negligence and medical racism, where we have a group of white doctors that think that they know what is best for Black bodies and Black babies,” Doyley said in the hearing.
Both the doctors and Doyley mentioned recommendations from the American College of Obstetricians and Gynecologists. However, neither one cited the organization’s stance on court-ordered C-sections, which the group has deemed to be “ethically impermissible.”
“A lot of that comes from medical negligence and medical racism.”
After three hours of testimony — all while Doyley lay in her hospital bed — the judge ruled that she could keep laboring unless there was an emergency. If that happened, the hospital could operate, whether she wanted it or not. The judge would reconvene the hearing in the morning.
In response to questions from ProPublica, Kalil wrote in an email that the judicial code of conduct prohibits judges from commenting on cases. “These ethical standards exist to protect the integrity of the judicial process, ensure fairness to all parties, and preserve the Court’s neutrality,” he wrote.
Overnight, doctors said the baby’s heart rate dropped for seven minutes. Doyley awoke to find herself being wheeled in her hospital bed into surgery. She called out to her sister who was asleep in the hospital room.
“I had to tell her, ‘Hey, wake up,’” Doyley said. “‘Something is going on.’ She’s trying to put on her shoes. I’m like, ‘Girl, leave the shoes. Let’s go.’”
Doyley recalled reciting a short prayer as her sister scrambled into the operating room. The baby was delivered by C-section. Although Doyley’s daughter was initially limp, she perked up and became responsive within a few minutes. Doctors took her to the NICU while Doyley went to recovery. And to get ready to face the judge again.
At the 8 a.m. hearing, Doyley looked pained and groggy. She told the judge she still hadn’t been allowed to see her daughter and asked if he could help. A doctor testified that the baby had been brought to the NICU in respiratory distress and placed on a machine to help with her breathing.
Kalil said he couldn’t order the hospital to do anything. The matter he had been appointed to hear involved only her unborn baby. He had no authority over the child in the nursery.
Kalil wished her well and quickly closed the case.
The post They Didn’t Want to Have C-Sections. A Judge Would Decide How They Gave Birth. appeared first on Truthdig.
-
Stay at home advice questioned and rules too tough – key findings from Covid report
An NHS close to collapse, patients failed and NHS staff put at risk – what you need to know.