From Ebola outbreaks in Central Africa to the complex evacuation of passengers aboard a hantavirus-stricken cruise ship, the UN World Health Organization (WHO) opened its annual assembly on Monday as countries grapple with disease outbreaks, deep funding cuts and growing geopolitical tension.
Blog
-
LGBTIQ+ face mounting violence and discrimination, warns UN rights chief
Violence and discrimination against LGBTIQ+ people are widespread, including at school, where 45 per cent of LGBT youth report being bullied. -
Ebola outbreak follows hunger and displacement crisis in DR Congo
A day after the World Health Organization (WHO) declared the new Ebola outbreak in eastern Democratic Republic of the Congo an international emergency, top global disease transmission experts stressed that the chances of another global pandemic similar to the 2019 coronavirus emergency are increasing all the time. -
Ex-Zelensky Aide Posts $3.2 Million Bail in Money-Laundering Case
Andriy Yermak, the former chief of staff to Ukrainian President Volodymyr Zelenskyy, may soon be released from pretrial detention after the equivalent of $3.2 million bail was posted on his behalf, according to Ukraine’s state news agency UNIAN reported which cited the High Anti-Corruption Court.
Yermak, who has denied any wrongdoing, was jailed on May 14 pending an investigation into a $10.5 million money-laundering scheme tied to the construction of a luxury residential complex near Kyiv. The charges stem from a broader anti-corruption probe into alleged wartime kickbacks.
-
Interpol Arrests Over 200 in Sweeping Middle East and Africa Cybercrime Crackdown
In a first-of-its-kind crackdown across the Middle East and North Africa, Interpol announced Monday that authorities have arrested 201 individuals linked to cross-border cybercrime networks.
Code-named “Operation Ramz,” the coordinated effort spanned 13 countries and was aimed at neutralizing costly phishing, malware, and cyber scam operations. Along with the arrests, law enforcement officials seized 53 servers while identifying 382 additional suspects and 3,867 victims.
The operation involved authorities from Algeria, Bahrain, Egypt, Iraq, Jordan, Lebanon, Libya, Morocco, Oman, Palestine, Qatar, Tunisia, and the United Arab Emirates.
-
A blast from the past: The “interstitium,” the inspiration for that recent awful NYT acupuncture article
I’m on vacation this week and decided to repost a 2018 article that I had written for my other blog (but never published on SBM) that’s oddly relevant to the SBM post last week about that awful NYT acupuncture article. Meet the introduction of the “interstitium” in acupuncture, complete with a major Deepak Chopra connection!
The post A blast from the past: The “interstitium,” the inspiration for that recent awful NYT acupuncture article first appeared on Science-Based Medicine.
-
24th June: Neurodiversity: Liberation or Trap? with Professor Sami Timimi.
 Wednesday 24 June • 6 PM – 7:30 PM GMT+1Overview
Wednesday 24 June • 6 PM – 7:30 PM GMT+1OverviewJoin Professor Sami Timimi for a rare space to think critically about today’s powerful and rapidly spreading neuro narrative.
The idea of neurodiversity has become one of the most influential and widely discussed concepts in today’s mental health culture. For many, it offers recognition, belonging and a powerful challenge to deficit based thinking. For others, questions are beginning to emerge about how the concept is being used and whether it may sometimes unintentionally reinforce the very ideas it set out to challenge.
In this thought provoking workshop, Professor Sami Timimi invites us into a rare space to reflect critically and compassionately on these issues. Drawing on ideas from his recent book Searching for Normal: A New Approach to Understanding Mental Health, Distress and Neurodiversity (2025), Sami will explore the promises, tensions and possible unintended consequences surrounding the rise of neurodiversity discourse.
Expect a thoughtful, respectful and stimulating 1.5 hours about one of the most important debates shaping our culture today.
The post 24th June: Neurodiversity: Liberation or Trap? with Professor Sami Timimi. appeared first on Mad in the UK.
-
Ebola outbreak in Central Africa declared a ‘Public Health Emergency of International Concern’
The World Health Organization (WHO) has declared the ongoing Ebola outbreak in the Democratic Republic of the Congo (DRC) and Uganda a Public Health Emergency of International Concern, citing rising cases, cross-border spread and significant uncertainties about the scale of the epidemic. -

Lithuania Pitches Pirate Site Blocking as Defense Against “Hybrid Warfare,” Including Russian Disinformation
The Radio and Television Commission of Lithuania (LRTK), the Baltic country’s media watchdog, has been one of Europe’s most active anti-piracy enforcers.
In recent years, it blocked hundreds of domains and thousands of IP addresses, fined users without going to court, and froze bank accounts tied to pirate operations.
Next month, LRTK will share some of its hard learned lessons in Geneva. At a meeting of the World Intellectual Property Organization’s Advisory Committee on Enforcement (ACE), LRTK’s Andrius Katinas will describe the Lithuanian approach as a template for other countries.
According to the contribution, which is publicly shared in advance of the June meeting, copyright enforcement in Lithuania is no longer just about copyright. It is “a method of hybrid warfare,” which can also counter Russian disinformation and safeguard the privacy of citizens.
Russian Disinfo as a “Hybrid Threat”
The hybrid-threat framing rests on two separate claims, which both are unrelated to copyright infringement. The first is that pirate IPTV services can, willingly or not, be used as distribution channels for Russian propaganda.
LRTK explains that many of the IPTV services it monitors operate from hostile countries and retransmit Russian state channels, which are sanctioned and formally banned by the European Union.
“Those channels include EU-sanctioned outlets that not only spread propaganda and disinformation, but also broadcast numerous national channels and live sports without the consent of the rights holders.”
“In blocking broadcasts because of copyright infringement, the Commission also blocks access to hostile information (and vice versa), which is a method of hybrid warfare,” LRTK’s abstract of the upcoming presentation reads.
A Blocked IPTV channel 
As a direct neighbor of Russia, Lithuania has been very active in taking down Russian disinformation. In addition to blocking numerous sites and services, LRTK also fined hosting provider UAB Melbikomas €10,000 for breaching EU sanctions by hosting more than 50 sports channels.
Filmai.in and other Privacy Threats
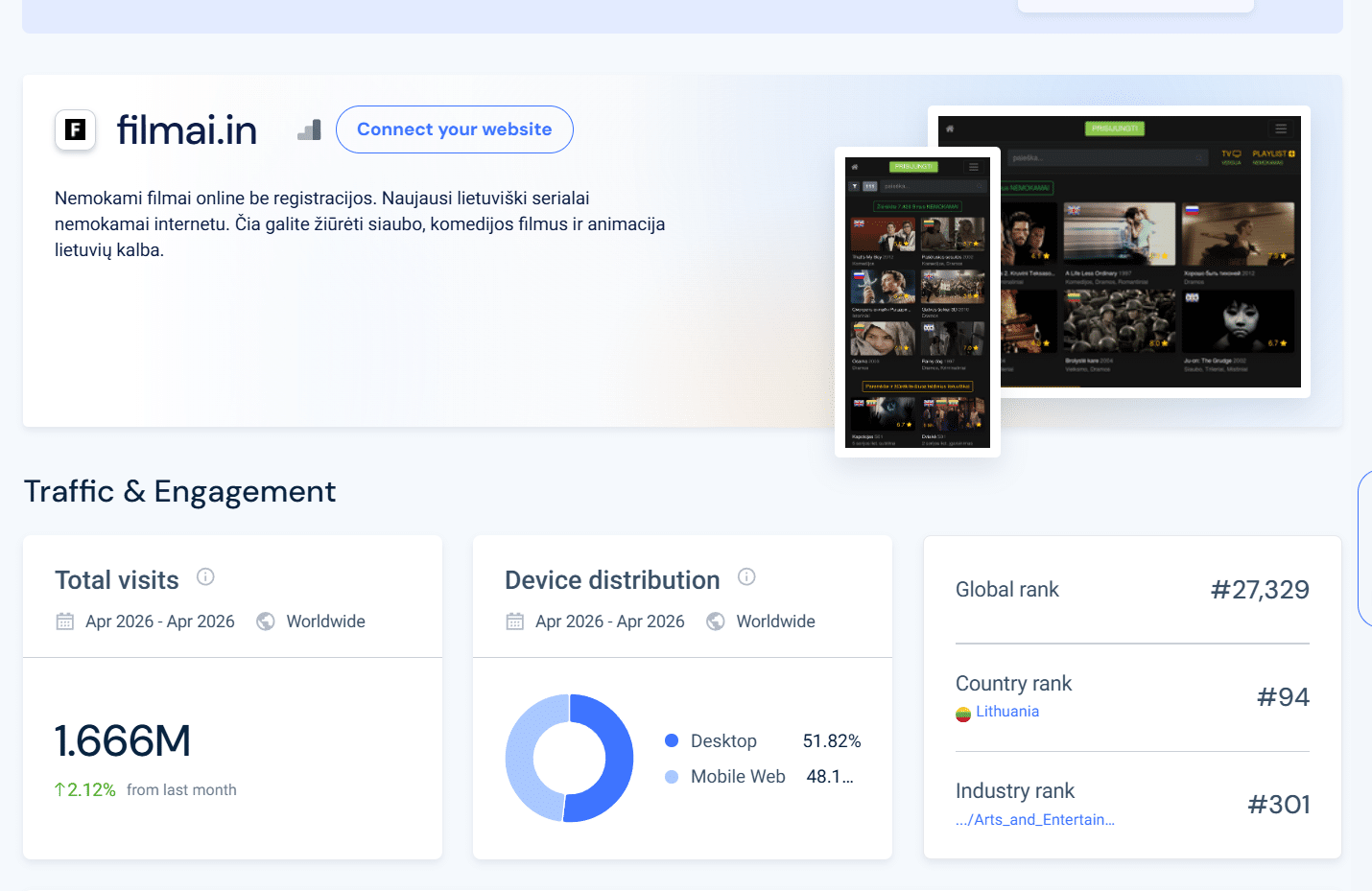
Pirate site blocking can also serve another purpose, as it prevents potential security breaches. Lithuania has experience with this, as user data of the popular local pirate site Filmai leaked online, including 645,000 email addresses, usernames, and plain text passwords.
This breach happened more than 5 years ago, and blocking the site does not remove the leaked data from the darknet. However, it may help to limit the fallout of future breaches at Filmai or other pirate sites.
These privacy issues are a serious concern, LRTK notes, stressing that pirate sites generally don’t have the best security.
Leaked credentials end up on the dark web, with LRTK suggesting that they can be picked up by hostile-state cyber groups for use in operations against state institutions and strategic companies. And since credentials of government officials have also been found in the Filmai leak, state security might become an issue.
“It has even been found that Government officials had registered on the Filmai website using official email addresses, creating security concerns, such as the potential for unauthorized access to State institutions, the signing of documents, or responding to residents’ inquiries,” LRTK writes.
Filmai is blocked now, and one of the administrators of the site was convicted in 2023. However, the site itself remains online and, according to Similarweb, it remains among the top 100 visited sites in the country.
The Lithuanian Model
LRTK explains that it has broad experience with fighting piracy threats, using a wide variety of OSINT skills. It specifically mentions tools such as domaintools.com, oxylabs.io, epieos.com, Wireshark, and SimilarWeb, which help to identify perpetrators or monitor for illegal activities.
In recent years, the watchdog has blocked more than 400 domains and 7,000 IP addresses. In addition, it imposed fines in over 250 cases since 2023.
Much of this blocking system is centralized and automated. When LRTK identifies a new site, or a mirror of a previously blocked site, a blocking instruction is sent to all Internet service providers. Within twenty minutes, the domain or IP is blocked across the country.
LRTK has also frozen bank accounts linked to pirate operations, delisted URLs from Google Search, removed advertisements from pirate sites, and suspended illegal IPTV apps from Google Play and the Apple App Store.
The Dutch Export Problem
According to the presentation, Lithuania’s experience can “serve as a model for other national authorities and rights holders”. While that may be true, a Dutch example should show that blocklists should not be copied blindly.
In December 2025, the Dutch ISP trade association NLconnect tried to help ISPs by compiling a master blocklist, to comply with the EU’s ban on Russian disinformation. Because the Dutch government did not provide guidance, it compiled a reference blocklist of 797 domains, using blocklists from regulators in Germany, Austria, Estonia, Finland, and Lithuania.
As we reported at the time, this effort resulted in some unexpected blocks. Dutch users of Ziggo lost access to ShareChat, India’s largest homegrown social media platform with hundreds of millions of users. The same applied to Odysee.com, online radio aggregators Streema and Viaway, and various pirate IPTV domains including IPTV-home.net, Ottclub.tv, and Limehd.tv.
Most of those domains traced back to a single source: LRTK’s blocklist.
Responding to the issue, the Dutch regulator ACM informed us in December that it does not monitor the actual execution or the content of the sanctions list. However, after ISPs started to complain as well, ACM formally investigated the matter, concluding that LRTK’s blocklist is too broad for the Netherlands.
As reported by Tweakers in February, ACM eventually concluded that the Lithuanian list had been compiled under both the EU sanctions regulation and a broader Lithuanian national law banning Russian-financed television content.
This means that the Lithuanian list is not usable outside Lithuania, and NLconnect dropped the entire Lithuanian source list, shrinking their reference list from 797 domains to 335.
The Dutch overblocking example can’t be blamed on Lithuania, but it shows that when it comes to cross-border blocking efforts, caution is warranted. In any case, it is clear that blindly copying third-party blocklists is not the best approach.
—
The WIPO contribution, “Combating Digital Piracy: Strategic Enforcement through DNS/IP Blocking and OSINT Tools,” is available here (pdf).
From: TF, for the latest news on copyright battles, piracy and more.
-
Trying to rebut inconvenient truths: a reply to Aftab’s comments on models of drug action.
Summary: Aftab tries to rebut my work on theories of drug action, but he cannot muster any substantive arguments. He wants to obscure the important difference between taking a drug that targets a biological mechanism and taking a psychoactive substance whose global mental and physical alterations may temporarily suppress or obscure symptoms.
I started this blog a while ago in response to Awais Aftab’s blog on my theory of models of drug action. I can’t remember why I put it aside but since it remains one of the few serious attempts to engage with my work on this, I thought it was worthwhile finishing.
I am genuinely grateful to Aftab for taking this work seriously, when, as he says himself, the majority of the academic psychiatric community continue to ignore it. I think this is telling, as is the fact that Aftab can’t offer any substantive arguments against my thesis of drug action despite clearly wanting to. Nevertheless, the questions he raises highlight the importance of questioning how we understand the nature and action of psychiatric drugs and the consequences of getting this wrong.
I also want to thank Aftab for clarifying that the distinction between the drug-centred and the disease-centred models of drug action is not a matter of whether a drug acts ‘symptomatically’ or on fundamental disease mechanisms. The disease-centred model is the idea that drugs work by targeting specific biological mechanisms that generate the symptoms of a disease or disorder. Disease-centred drugs can act on the origin of the disease, like an antibiotic, or they can act on the physiological mechanisms that produce symptoms, such as the way that salbutamol relieves wheezing in asthma by counteracting the airways constriction. It doesn’t treat the original cause of the asthma, so in this sense it is a symptomatic treatment, but it works on the biological mechanism that provokes the symptom and in this way it is acting in a disease-centred way.
The drug centred model, by contrast, highlights the fact that psychiatric drugs are psychoactive substances that produce global alterations to mental states by changing the normal state of our brain chemistry and activity. In this respect they are the same as alcohol and other recreational drugs, but, of course, each drug is different and produces different sorts of mental changes and the changes do not have to be pleasant or appealing. Psychiatric drugs can make people, in general – and animals – drowsy, emotionally blunted, inhibited, overactive or disinhibited, depending on the type of drug and dose, along with various other effects. When they are taken by someone who is in a state of distress, mania, depression or psychotic confusion, the changes they induce will be superimposed onto to the individual’s symptoms and in some cases mask or suppress them. The drug-induced effects may be helpful or they may not be, but this is how a psychoactive substance should be assumed to be acting on our mental states until proven otherwise.
Mainstream psychopharmacology, however, which simply assumes that drugs work in a disease-centred way, characterises these effects as side effects and considers them of little intrinsic interest. It is a total tragedy that the billions of dollars that have been poured into psychopharmacology research over the last few decades have not been used to develop our knowledge of how psychiatric drugs change our normal physical and mental functions and the consequences that can have.
Now to Aftab’s problems with the drug-centred approach.
Number 1 on his list of problems is his correct clarification that the ‘drug-centred’ model is not just saying that psychiatric drugs are symptomatic rather than disease-modifying treatments. Pain killers are symptomatic but target the biological mechanisms of pain and painkillers such as aspirin or paracetamol do not have psychoactive effects (unlike opiates, which do), they do not change one’s level of consciousness, emotions or thinking processes. Alcohol, on the other hand, affects pain mainly in a drug-centred way because when you are intoxicated you are less aware of pain. The effects of alcohol are superimposed onto the pain – they do not modify its productive mechanism.
Number 2 says: ‘it is obvious that an interaction between psychoactive effects and psychiatric symptoms at the psychological level must also involve an interaction of some sort between psychoactive effects and psychiatric symptoms at the physiological level.…’
But the issue at stake is what sort of interaction occurs at the physiological level between the drug and the symptoms. If you take a drug that knocks you unconscious, you can’t feel depressed or anxious or have psychotic experiences but this doesn’t mean the drug is targeting the mechanisms that are assumed to underpin these conditions. The global alterations produced by drugs can, and usually will, affect mental activity, including psychiatric symptoms or syndromes, without having to exert an effect on a specific and hypothetical symptom-generating mechanism.
Number 3 is not an objection to the drug-centred model. It is an expression of Aftab’s frustration. He says: ‘Accepting the drug-centered model imposes a severe restriction on what sorts of hypotheses we can consider to explain the mechanisms of psychiatric medications. The only kosher mechanisms are those that invoke effects such as sedation, cognitive slowing, and emotional blunting, because the possibility of psychiatric medications having any direct effects on mechanisms and processes related to symptoms is dismissed as “disease centered.”’
What Aftab is essentially saying here is that the drug-centred model gets in the way of hypothesising about possible biological mechanisms of symptom causation. This might be why the rest of the psychiatric community has assessed that the only way to cope with the drug-centred model is to ignore it.
Number 4 ‘The difference between acting on a psychological mechanism that produces symptoms and a psychoactive effect that suppresses symptoms is a conceptually important one, but the drug-centered account doesn’t seem to have the conceptual resources to articulate it.’
I am not sure that I understand the problem here. If a drug reduces ruminations or psychotic experiences because it numbs emotional responses and slows up thought processes in general (in the way that antipsychotics were thought to act by their early proponents, by the way) then surely we have a situation in which the psychoactive effects of a drug result in the reduction or suppression of ‘symptoms’?
Number 5 reads: ‘In addition to mechanisms that produce symptoms, we can also talk about mechanisms that sustain symptoms (once they are generated) and mechanisms that influence symptoms (in terms of severity or quality). The more such mechanisms exist and the more they are likely targets of psychiatric medications, the less support there is for the idea that psychotropics do not act on symptom mechanisms.’
The problem is that specific biological mechanisms that produce what we call psychiatric symptoms or syndromes, or that sustain or maintain them have not been demonstrated. They remain hypothetical and therefore cannot be targets of psychiatric medication.
Number 6 It allows for a sort of motte-and-bailey argument where “the medication doesn’t correct a dysfunction” (the motte) is taken to assume “the medication works by blunting/numbing/masking your symptoms” (the bailey), and when the bailey is challenged, the person simply retreats to the motte without changing their views and while continuing to assert the bailey any opportunity they get.
This point highlights how different our perspectives really are. As I highlighted above, the drug-centred approach starts from the undisputable fact that psychiatric drugs are drugs that enter the brain and change the way it normally works. This is likely to affect our mental activity – to change our thoughts, emotions and behaviours in more or less subtle ways (traditionally of no interest to mainstream psychopharmacology). These changes may or may not be useful in certain situations (‘work’), and they may be liked or disliked. This is how a psychoactive substance should be assumed to be acting on our mental states until proven otherwise.
But Aftab and many other psychiatrists assume that drugs must act on a symptom-generating, biological mechanism, even if we haven’t found any such mechanism, and that the brain and mind-changing effects of the drugs are irrelevant or incidental. This assumption is not justified by the inconsistent findings that have emerged from decades of highly funded psychopharmacological research. If you do enough studies, and there have been tens if not 100s of thousands of studies looking for the biological underpinnings of psychiatric disorders, you will find something, but no clear mechanisms have emerged. This is why our serotonin paper was important. The idea that depression is caused by low levels or activity of serotonin has been one of the principal theories of the biological causation of a mental disorder and subject to decades of research in different areas using different techniques. It has not been proven. In fact the evidence is weak and highly inconsistent. And none of the other numerous hypotheses about the presumed biological origins of depression or depressive symptoms have been demonstrated either.
Number 7 The idea that psychiatric medications simply numb or suppress painful emotions – essentially no different from consuming alcohol – can veer dangerously close to a moral stance towards psychopharmacology, even if this is unintended. Such danger is particularly acute when it is believed that “what we characterize as mental illness, therefore, refers not to an illness or disease, but to patterns of unusual but still essentially self-directed behavior. These patterns can be understood as aspects of character…” as Moncrieff does.
It is not a question of moral judgement. It is a question firstly of informed consent (letting people know what the drugs do and don’t do) and secondly of whether it is actually useful to take mind-altering substances, particularly ones with numbing effects. If someone is acutely psychotic, then the mental slowing and numbing effects of antipsychotics might be helpful. If someone is distressed, is it useful for them to be numbed? I can see it might enable them to function better and get on with doing things that are likely to be helpful. On the other hand, we recognise that when people do this with alcohol and other illicit drugs, at least on a continual basis, it doesn’t usually work out like that.
Number 8 Medications often work in ways that are independent of the existence of any “disease” process, but that is as true of general medicine as it is of psychiatry. We still have to figure out what effects medications have (which span across neurobiology, cognition, phenomenology, etc.) and how these effects modify and interact with the mechanisms and processes involved in the generation or maintenance of the particular clinical state we are trying to address. These interactions are complex and only inadequately classified as either “disease centered” or “drug centered.” As is the case with other Szaszian binaries, the illusion only works if you accept the binary at face value.
Aftab is correct to the extent that all drugs, whether used for depression, breast cancer, asthma or epilepsy change the normal state of the body. However, in general medicine, we usually have a pretty good idea of how a drug impacts particular disease or symptom generating-mechanisms. Taking the example of asthma, as I explained above, salbutamol is known to reduce wheezing by relaxing the constricted airways in the lungs. Treating wheezing in a drug-centred way might involve giving people diazepam or alcohol to produce general relaxation, which, while having no specific bronchodilation effects, might help them feel less stressed and prevent their stress making the situation worse.
This example highlights how using drugs in a drug-centred way is a pretty crude business. Indeed, modern medicine has by and large been about replacing this approach with specific, disease or mechanism-targeting treatments. I think this is the rub. Psychiatrists don’t want to be left out. They want to have sophisticated treatments like their general medical colleagues. But they don’t. They have crude but sometimes useful or necessary tools for modifying people’s feelings and behaviour. Pretending otherwise has just left psychiatry woefully ignorant about the tools it uses.
Aftab then proposes four other approaches for understanding the nature and action of psychiatric drugs. However, none of them amount to a theory about how the drugs act and they seem more like a plea to ignore the issue.
“Effects-centered psychopharmacology” is a suggestion to explore the effects of drugs without committing oneself to any position about how these might influence symptoms. “Phenomenological psychopharmacology” is the same thing but presumably with more emphasis on the mental or behavioural effects. “Outcome-centered psychopharmacology” is the idea that we should just concentrate on the outcomes of drug treatment and not try and understand how it produces the effects it does. And “Iatrogenic psychopharmacology” is simply a plea to pay attention to adverse effects, which is, of course, welcome.
All these proposals imply that it is not important how a drug achieves its effects, but I strongly disagree. There is a world of difference between taking a drug to correct a biological abnormality and taking something that works, if it does, by interfering with normal brain chemistry and activity. The first sounds like a good thing, other things being equal, the second sounds dicey, and generally is. Fiddling about with brain chemistry without knowing what we are doing has had disastrous results for tens of thousands of people around the world (and these are just the ones we know about through online fora) who have been plunged into severe and prolonged withdrawal states or experience persistent sexual dysfunction after taking antidepressants, to mention just a couple of examples.
Aftab’s claim that the distinction between the drug and disease-centred models is not important, or is a problematic ‘binary,’ prevents people from being properly informed about the nature of the drugs they are offered for mental health problems and the risks they run in taking them.
{kind=link}